People often wait for a dramatic collapse before they take drinking seriously. That is the mistake. The pattern usually starts smaller: someone is irritated when a partner mentions alcohol, someone keeps promising they will cut back, someone starts drinking earlier in the day and calling it “just a habit”. None of that proves addiction on its own, but it is the sort of behaviour that clinicians are trained to notice.
That is where the CAGE questionnaire comes in. It is short on purpose. Four questions. No long history, no complicated scoring, no attempt to play therapist. It is designed to catch a problem early enough that a proper conversation can happen before the situation gets more dug in.
What CAGE Actually Does
CAGE is a screening tool, not a diagnosis. That distinction matters because people love to treat a quick questionnaire like a verdict. It is not that. It is a first pass used in clinical settings to flag possible alcohol misuse, especially in primary care where time is limited and denial is common.
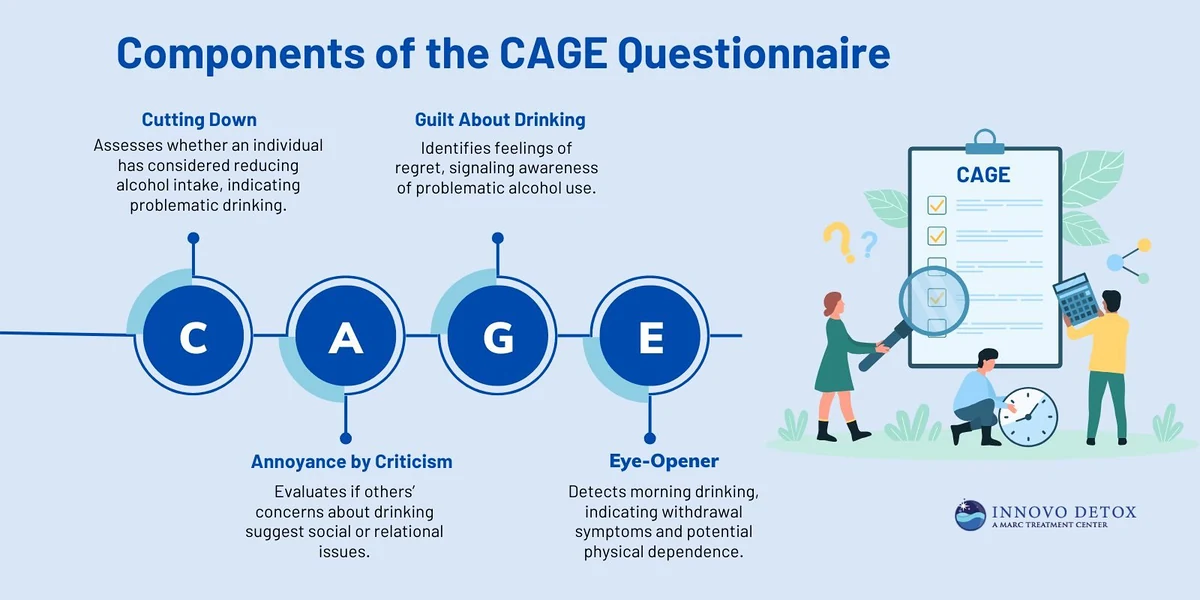
The name comes from the four themes behind the questions:
- Cut down
- Annoyed by criticism
- Guilty feelings
- Eye-opener
Each item is answered yes or no. There is no scoring nuance hidden in the wording, and no trick to it. If someone says yes, that answer counts. If they say no, it does not.
The point is not to catch every possible drinking problem with perfect detail. It is to spot a pattern that justifies a closer look. In practice, that means CAGE is useful when alcohol is starting to affect relationships, mood, health, work, or the simple ability to function without a drink.
The Four Questions, Unpacked
Cut down
The first question asks whether a person has felt they ought to reduce their drinking.
That sounds basic, but it is doing real work. People who are drinking in a healthy or controlled way usually do not spend much time privately negotiating with themselves about whether they should stop. The thought of cutting back starts appearing when drinking is no longer fully under choice. Someone may still be functioning, still getting to work, still telling themselves it is manageable. But the fact that they are even asking the question internally is worth noticing.
This is often the first honest crack in the story. Not “I drink too much”, because people rarely say that out loud at first. More often it is: “I should probably slow down.” Then they do not.
Annoyed by criticism
The second question asks whether other people have annoyed them by criticising their drinking.
That irritation is not the real issue. Lots of people hate being criticised. The question is whether drinking has become visible enough that other people are noticing and reacting. Partners, friends, children, colleagues, siblings. Once criticism starts, it usually means the drinking has stopped being private.
People often dismiss this question because they think, “Everyone has an opinion.” Sometimes that is true. Sometimes the criticism is clumsy or unfair. But repeated concern from people close to the drinker is not nothing. It may be the first external sign that the problem is getting larger than the person wants to admit.
Guilty feelings
The third question asks about guilt linked to drinking.
Guilt is slippery because it can mean different things. Some people feel guilty after a binge, after a row, after missing family time, after spending money they did not mean to spend. Others feel guilty because they know the drinking is out of step with their values, even if they cannot stop. Either way, guilt suggests a split between what someone says they want and what they keep doing.
This question matters because addiction often survives on that split. A person can look calm on the outside and still carry a private sense that something is not right. They may be ashamed, defensive, or tired of hearing themselves promise change. That emotional load is part of the picture, not a side issue.
Eye-opener
The fourth question is the one people remember because it is blunt: have they needed a drink first thing in the morning to steady nerves or get rid of a hangover?
That is not casual drinking. It points towards dependence. When alcohol moves from being something a person wants to something they need to feel normal, the body has started to adapt to it. Morning drinking often means withdrawal is already happening, even if the person calls it “taking the edge off” or “sorting myself out”.
This is usually the question that makes people uncomfortable, because it removes the argument about style and gets to physiology. If someone needs alcohol early in the day to function, the issue is no longer just social or behavioural. It has become physical as well.
How Scoring Works
Each yes answer scores one point. Zero to four is the total range.
A score of two or more is generally treated as a positive screen. That does not mean the person definitely has alcohol dependence. It means the pattern is concerning enough that further assessment is warranted.
That distinction is not academic. People often hear “positive” and assume diagnosis. In medical screening, positive means “look closer”, not “case closed”. CAGE is useful because it is quick and it tends to pick up problems that are easy to miss in ordinary conversation.
The questionnaire has been reported to have high sensitivity and specificity, around and respectively, for identifying alcohol-related problems. In plain English, that means it has been shown to do a decent job of flagging people who may genuinely have an issue, while not crying wolf constantly. But those figures do not turn it into a full diagnostic tool. No screening tool does that on its own.
What A Positive Result Means
A result of two or more yes answers suggests a high likelihood of alcohol misuse or dependence and should prompt a proper clinical assessment.
That next step matters more than the score itself. A clinician can put the answers into context. Is the person drinking heavily every day, or only in episodes? Are there signs of withdrawal? Is alcohol affecting sleep, blood pressure, mood, relationships, work, or safety? Are there other substances involved? Is the drinking a cause, a symptom, or both?
This is why CAGE was built for clinicians in the first place. It is a quick screen, not a self-help quiz. Someone can answer honestly and still misunderstand what the result means. They might underplay it, or panic, or decide they are “fine” because they only scored one. None of those reactions is reliable enough to guide treatment.
If you are worried about a partner, parent, sibling, or adult child, a positive screen is not a reason to argue harder. It is a reason to slow down and get the facts straight. For families looking beyond the UK, free CAGE test resources through Wedorecover can help frame the issue more clearly and point people towards alcohol rehab and support for families in South Africa without dressing the problem up.
Why Clinicians Still Use It
CAGE stays relevant because it is short and because it catches the kinds of answers people often give only when asked directly.
In a busy primary care setting, that matters. Alcohol problems are frequently hidden behind vague complaints: poor sleep, anxiety, low mood, stomach issues, repeated falls, missed appointments, relationship stress. A patient may not walk in saying, “I think I have a drinking problem.” They may walk in saying they are exhausted, or they are under stress, or they do not know why their blood pressure is up.
A compact screening tool gives the clinician a fast way to ask the awkward question without needing a ten-minute speech. It opens a door that may otherwise stay shut.
It is also worth saying that CAGE is not the only option. It is a blunt instrument. Useful, but blunt. That is not a criticism if you understand its purpose. In the same way a thermometer does not diagnose the cause of a fever, CAGE does not diagnose the cause of a drinking problem. It tells you the temperature is off.
CAGE-AID And Why It Exists
There is a modified version called CAGE-AID. The “AID” expansion broadens the same four questions so they can refer to alcohol or drug use.
The logic is straightforward. Some people do not have a single-substance problem. Alcohol and drugs are mixed together in ways that make the pattern harder to read if you only ask about one of them. CAGE-AID keeps the same structure, including the eye-opener question, but adapts the wording to include drinking or drug use first thing in the morning.
The scoring stays the same. A score of two or more is still clinically significant and still calls for a professional assessment. That similarity is useful because it keeps the tool simple. The risk, however, is that people start using it casually, as if it were a label machine. It is not. It is a prompt for action.
What Not To Do With The Result
Do not use CAGE to diagnose yourself.
That warning is not there to be dramatic. It is there because self-assessment goes wrong in both directions. Some people minimise. Some catastrophise. Some answer the questions according to how they feel that day rather than how they have actually been living. A professional can separate the guilt, the denial, the bargaining, and the facts. A person answering alone usually cannot.
A positive screen should lead to a conversation with a healthcare professional, not a private internet spiral. A proper assessment may look at drinking history, withdrawal symptoms, mental health, physical health, medications, and social consequences. From there, the right UK alcohol treatment options and support can be discussed in a way that fits the actual situation rather than a guess.
Cost is part of that discussion too. People avoid asking about treatment because they assume it will be unaffordable. Sometimes it is, sometimes it is not. That question should be raised early. If insurance is involved, it may cover all or part of treatment, and it is better to ask than to assume the worst and do nothing.
For readers comparing treatment contexts internationally, alcohol rehabs news from alcohol-rehabs.co.za can give broader context on how rehab is discussed and delivered beyond the UK, which is useful when family members are trying to understand the wider landscape rather than one local service.
The Part Families Usually Miss
Families often fixate on whether the person is “bad enough” for treatment.
That is the wrong test. The more useful question is whether the drinking pattern is already causing harm and whether it is likely to keep going if nobody interrupts it. CAGE helps because it pulls the conversation away from moral judgement and towards observable signals: inability to cut down, irritation when challenged, guilt, and morning drinking.
Those are not personality quirks. They are warning signs.
The hardest truth is that many people do not seek help because they have had a dramatic rock-bottom event. They seek help when the damage becomes hard to keep explaining away. CAGE is designed to catch that stage. Not the film version. The ordinary, messy, halfway stage where the excuses are thinning out but the denial is still active.
That is also why family support matters. A relative does not need to become a clinician to notice a pattern and start a serious conversation. They do need to stop pretending the pattern is invisible.
For some families, especially those looking for practical guidance outside the UK, Innovo Detox Pennsylvania can be a useful point of comparison when thinking about how detox and treatment services are framed in other places, even if the final treatment plan stays local to the person’s needs.
Why This Matters Before Treatment Starts
Alcohol treatment works better when the problem is named early and honestly.
That does not mean every person with one positive answer needs rehab. It does mean a positive CAGE score should not be brushed aside as “just a bit of stress” or “a phase”. If the score is 2 or higher, there is enough evidence to justify a proper assessment. From there, someone can look at outpatient support, detox, counselling, structured rehab, or family intervention depending on severity and risk.
The value of CAGE is that it helps people stop arguing with the obvious. Not every problem drinking pattern looks dramatic. Some are tidy on the surface. Bills still get paid. Work still gets done. The person still jokes, still hosts, still functions. Then they need a drink in the morning, or they are angry when challenged, or they are privately ashamed of how dependent things have become.
That is the point where the screen is useful. It does not solve the problem. It names it.
Where To Land With It
If the questions hit a nerve, that is the signal. Not to panic, and not to pretend the result is meaningless. It is a prompt to get a real assessment from someone who can tell the difference between risky drinking, dependence, and something more complicated.
The CAGE questionnaire is brief because the first step often has to be brief. The real work starts afterwards. If two or more of the four questions land, the sensible move is not debate. It is action.
So the question is simple: if someone in front of you answered yes to cut down, criticism, guilt, or eye-opener, would you still call it harmless?